
You’ve probably heard two things about fertility and age that seem contradictory: that fertility falls sharply after 35, and that plenty of women have healthy pregnancies in their late 30s and beyond. Both are true. The reality is more nuanced than either headline suggests – and understanding the actual data makes it far easier to make decisions that are right for your life.
This article covers what’s happening to your fertility at 30, 35, and 40+: the biology that drives the change, what the statistics actually show, what tests can reveal about your individual picture, and what steps are available to protect your options.
A note before we start: the statistics in this article describe populations – averages across thousands of women. A 25% monthly conception rate doesn’t mean 1 in 4 months is guaranteed – it means that across a large group of women trying at this age, roughly 1 in 4 conceive in any given cycle. They don’t predict what will happen for any one person. If fertility timing or concerns are on your mind, a conversation with your OB/GYN or reproductive endocrinologist can give you a picture specific to you.
The Biology Behind Fertility and Age – Why It Matters
You Are Born With All Your Eggs
This is the fundamental difference between female and male fertility: men continuously produce new sperm throughout their lives. Women are born with all the eggs they will ever have.
At birth, a baby girl carries approximately 1 to 2 million immature egg cells (oocytes). By puberty, that number has already dropped to around 300,000 to 500,000. Over a reproductive lifetime, only about 400 to 500 eggs will actually be ovulated. The rest are lost through atresia – a continuous natural process of follicle death that occurs every day regardless of pregnancy, contraception, or menstrual cycles. Importantly: hormonal contraception, IUDs, and pregnancy do not pause or slow this process. The egg supply decreases continuously throughout a woman’s life1.
Two Things Decline: Quantity and Quality
As the egg supply decreases with age, two distinct effects occur:
Egg quantity (ovarian reserve) is the number of eggs remaining. This declines gradually throughout the 20s and 30s, then more steeply in the late 30s and 40s.
Egg quality (chromosomal integrity) refers to whether eggs can form genetically normal embryos. As eggs age, they accumulate DNA damage and are more likely to divide with chromosomal errors – a process called aneuploidy. This is the primary driver of rising miscarriage rates and falling IVF success rates with age. The frequency of these chromosomal errors accelerates significantly after age 352.
The two don’t always track together: a woman can have lower ovarian reserve but still-healthy egg quality. This is why ovarian reserve tests alone tell only part of the story.
Fertility by Age – The Data That Actually Matters
Fertility Statistics at a Glance
| Age | Monthly Conception Chance | Conceive Within 12 Months | Miscarriage Risk |
|---|---|---|---|
| Late 20s | 20-25% | ~85% | ~10% |
| At 30 | ~20% | ~75% | ~10% |
| At 35 | ~15% | ~66% | ~17-20% |
| At 40 | ~5% | ~44% | ~33-40% |
| At 45+ | <2% | Exceedingly rare; IVF with own eggs <5% per cycle (SART) | ~57-80% |
Sources: Tommy’s, Cleveland Clinic, Evidence-Based Birth, VARTA Australia
In Your 20s – Biological Peak
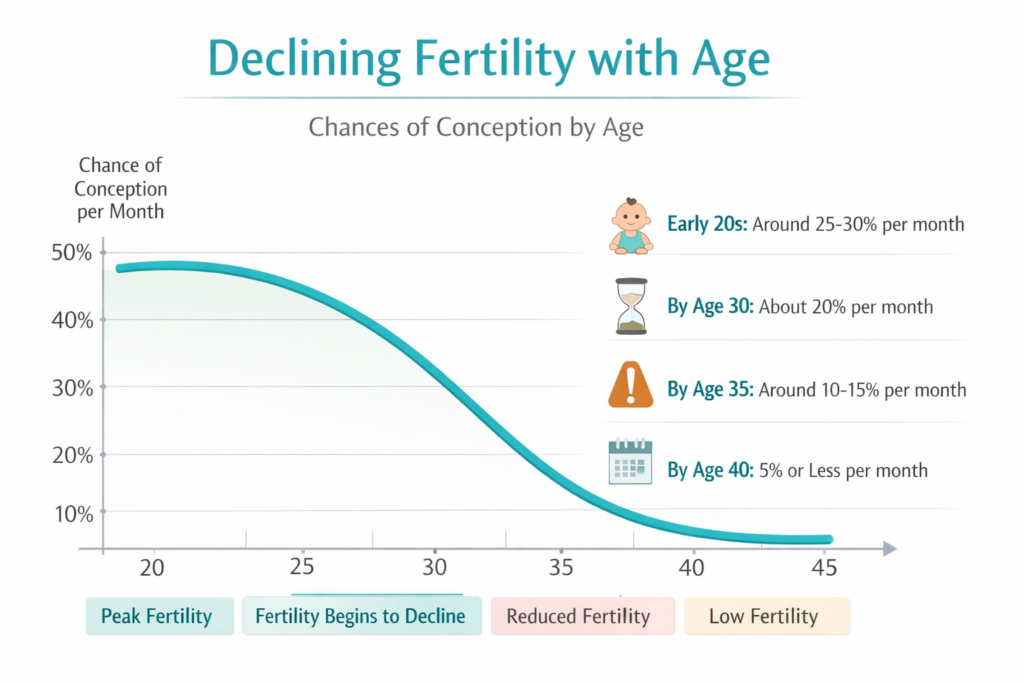
Monthly conception chance sits at 20-25%, and roughly 85% of women under 30 who are trying will conceive within 12 months3. Miscarriage risk is around 10-11%. Egg quantity and quality are both at their highest.
At 30 – A Gentle Decline Begins
Monthly conception chances remain around 20%, and approximately 75% of women conceive within 12 months. Miscarriage risk stays at around 10%. The typical AMH level at 30 is around 2.5 ng/mL – within the normal range.
The practical impact on natural conception at this stage is modest. The 30s are not the “beginning of the end” for fertility.
At 35 – The Acceleration Point
Monthly conception chances drop to around 15%, and approximately 66% of women – still a clear majority – conceive within 12 months. Miscarriage risk climbs to 17-20%, and around 35% of eggs are chromosomally abnormal (aneuploid)4. AMH averages ~1.4 ng/mL.
“Advanced maternal age” (AMA) is applied medically to pregnancies at 35 and older – a clinical flag for appropriate monitoring and screening, not a verdict that fertility has ended.
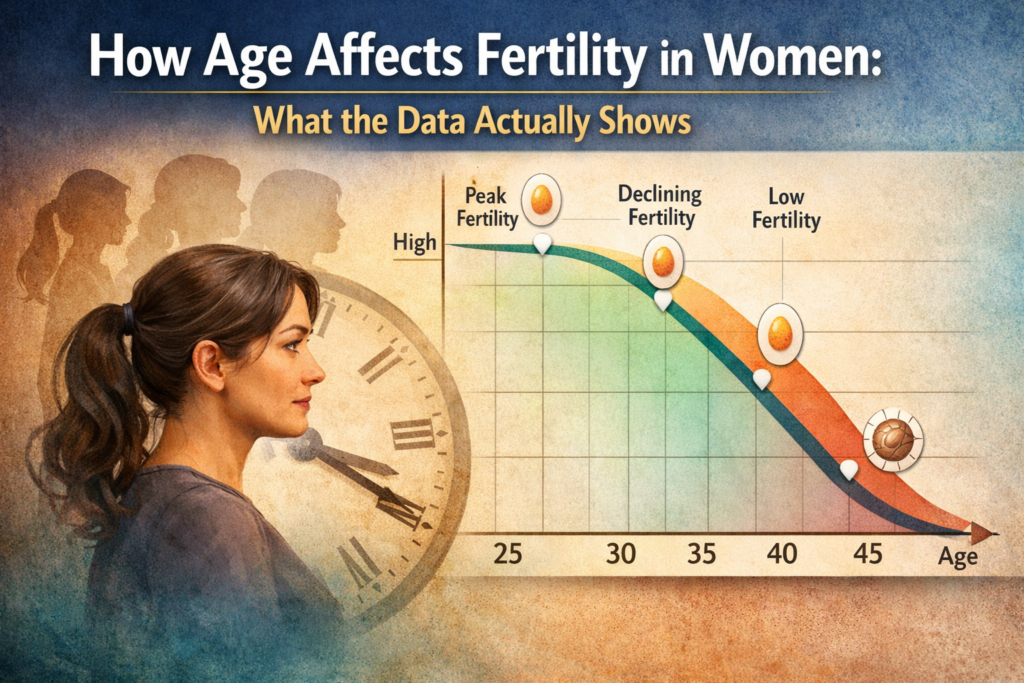
The phrase “biological clock” is real – but the image of a cliff is misleading. What the data shows is more like a slope that gradually steepens: meaningful change through the 30s, a more significant steepening after 35, not a sudden drop.
At 40 and Beyond – A More Significant Shift
Monthly conception chances are around 5% or less, and roughly 44% of women conceive within 12 months of trying. Miscarriage risk increases to 33-40%, and approximately 60% of eggs are chromosomally abnormal. Around 73% of women at 40 may have diminished ovarian reserve5.
Natural pregnancy at 45+ becomes exceedingly rare. For women using IVF with their own eggs at 44+, live birth rates per cycle are under 5% (SART data). Donor egg IVF – using eggs from a younger donor – becomes a more effective path for many women who want to carry a pregnancy.
Understanding Ovarian Reserve Testing
Ovarian reserve tests reveal the quantity of eggs remaining – not quality, and not a definitive pregnancy prognosis.
AMH Test (Anti-Müllerian Hormone)
The AMH test is a simple blood test done at any point in the menstrual cycle. AMH is produced by small follicles in the ovaries – higher levels generally indicate more follicles remaining.
Average AMH levels by age:
- At 30: ~2.5 ng/mL
- At 35: ~1.4 ng/mL
- At 40: ~0.5 ng/mL
A lower-than-expected AMH may suggest diminished ovarian reserve. But AMH measures egg quantity, not egg quality. Some women with low AMH conceive naturally. Others with normal AMH experience fertility challenges for unrelated reasons. AMH is most useful as a planning tool, interpreted alongside a full consultation.
Other Tests
- Day 3 FSH and Estradiol (E2): Elevated FSH on day 3 suggests the pituitary is working harder to stimulate the ovaries – a potential marker of lower reserve.
- Antral Follicle Count (AFC): Transvaginal ultrasound counting small visible follicles. More follicles = generally better reserve.
Pregnancy Risks That Increase With Age
Chromosomal conditions: The risk of chromosomal abnormalities like Down syndrome rises with maternal age:
- At 25: ~1 in 1,250
- At 35: ~1 in 353
- At 40: ~1 in 85
- At 45: ~1 in 12
Critical context: approximately 80% of babies with Down syndrome are born to mothers under 35 – because younger women give birth far more frequently overall. The risk percentage rises with age, but younger mothers make up the larger share of all births. Prenatal genetic screening (NIPT, amniocentesis, CVS) is offered regardless of age6.
Other complications more common with age include gestational diabetes, preeclampsia, and a higher likelihood of C-section. Absolute risk for any individual remains relatively low – but these factors explain why older pregnancies receive more frequent monitoring.
The anxiety of trying to conceive can itself affect hormone balance and conception. For more on that dynamic
What You Can Do: Proactive Steps
Know Your Numbers
An AMH test and antral follicle count give you a personalized baseline. Available through your OB, midwife, or a fertility clinic, these tests allow you to make decisions about timing and medical consultation with real data rather than assumptions – whether or not you’re actively trying.
Consider Egg Freezing if Planning to Delay
Egg freezing (oocyte cryopreservation) is most effective in the early-to-mid 30s when egg quality is relatively higher. Advances in vitrification (rapid freezing) have significantly improved outcomes. Egg freezing isn’t a guarantee – but it expands future options.
Lifestyle Factors That Support Egg Health
- Diet: A Mediterranean-style approach (whole grains, healthy fats, lean protein, abundant vegetables) supports egg quality. Folate, vitamin D, and omega-3 fatty acids are particularly relevant.
- Healthy weight: A BMI of 18.5-24.9 supports hormone balance and regular ovulation.
- Moderate exercise: Around 150 minutes of moderate activity per week. Excessive exercise combined with inadequate caloric intake suppresses ovulation.
- Quit smoking: Cigarette smoking directly accelerates egg quality decline – it is one of the most impactful modifiable fertility factors.
- Limit alcohol and caffeine; manage stress
- Prenatal vitamins: Starting folic acid (or methylfolate) 1-3 months before trying is recommended at any age.
Tracking your cycle becomes more valuable as monthly conception rates decrease.
When to Seek Specialist Help
- Under 35: Seek evaluation after 12 months of trying. Seek sooner if you have irregular or very short/long cycles, PCOS, endometriosis, prior miscarriages, or known fertility concerns.
- Ages 35-40: Seek evaluation after 6 months of trying
- Over 40: Speak with a reproductive endocrinologist before or very soon after you begin trying

Frequently Asked Questions
At what age does a woman’s fertility start to decline?
Fertility begins declining gradually in the early 30s, but the decline remains relatively modest until around age 35, when it accelerates. There is no sudden cutoff – it is a gradual curve that steepens over time.
Can you get pregnant naturally at 40?
Yes – approximately 44% of women age 40 trying to conceive do so within 12 months. Natural pregnancy at 40 is real and not rare, though it typically takes longer. Monthly conception chances are around 5%.
What is “advanced maternal age”?
Advanced maternal age (AMA) is a medical term for pregnancies in women 35 and older. It prompts discussion of monitoring and screening options – not a conclusion that pregnancy is especially risky or unlikely. Many women 35+ have entirely healthy pregnancies.
What does a low AMH mean for fertility?
AMH measures ovarian reserve (egg quantity, not quality). A low AMH for your age suggests fewer eggs may be available, but it does not mean natural conception is impossible. AMH is best used as a starting point for a conversation with a healthcare provider.
Does the father’s age affect fertility?
Yes – male factor infertility accounts for roughly 30% of fertility challenges. Sperm quality (motility, morphology, DNA fragmentation) does decline with age, particularly after 45. Paternal age is also associated with a small increase in certain genetic conditions7.
Is 35 too old to get pregnant?
No. At 35, approximately 66% of women conceive within 12 months – a clear majority. “Advanced maternal age” marks where the fertility decline steepens, not where it ends.
Final Thoughts
Age matters when it comes to fertility. But “matters” doesn’t mean “decides.” The majority of women at 35 conceive within a year; roughly half of women at 40 still conceive naturally; and understanding your specific situation through testing gives you far more to work with than age alone.
What you can control: knowing your numbers, supporting egg health through diet and lifestyle, and talking to a specialist at the right time.
The biology is real. And so is your ability to navigate it. The best time to start that conversation with your doctor is before concern becomes urgency.
- Cleveland Clinic – Female Fertility: Why Lifestyle Choices Count, https://my.clevelandclinic.org/health/articles/11779-female-fertility-why-lifestyle-choices-count
- RMA Network – Age and Egg Quality, https://www.rmanetwork.com/blog/egg-quality/
- Tommy’s – Fertility and Getting Pregnant, https://www.tommys.org/pregnancy-information/planning-a-pregnancy/fertility/age-and-fertility
- RMA Network – Age and Egg Quality, https://www.rmanetwork.com/blog/egg-quality/
- VARTA Australia – Age and Fertility, https://www.varta.org.au/resources/fact-sheets/age-and-fertility
- Mayo Clinic – Pregnancy After 35: Healthy Moms, Healthy Babies, https://www.mayoclinic.org/healthy-lifestyle/getting-pregnant/in-depth/pregnancy/art-20045756
- Evidence-Based Birth – Evidence on Age and Fertility, https://evidencebasedbirth.com/age-fertility/




![[variety of unsafe pregnancy foods including raw sushi deli meat soft cheese and raw eggs on a kitchen counter]](https://babiesparent.com/wp-content/uploads/2026/03/1_Unsafe_pregnancy_foods_202603301142-768x429.webp)
