
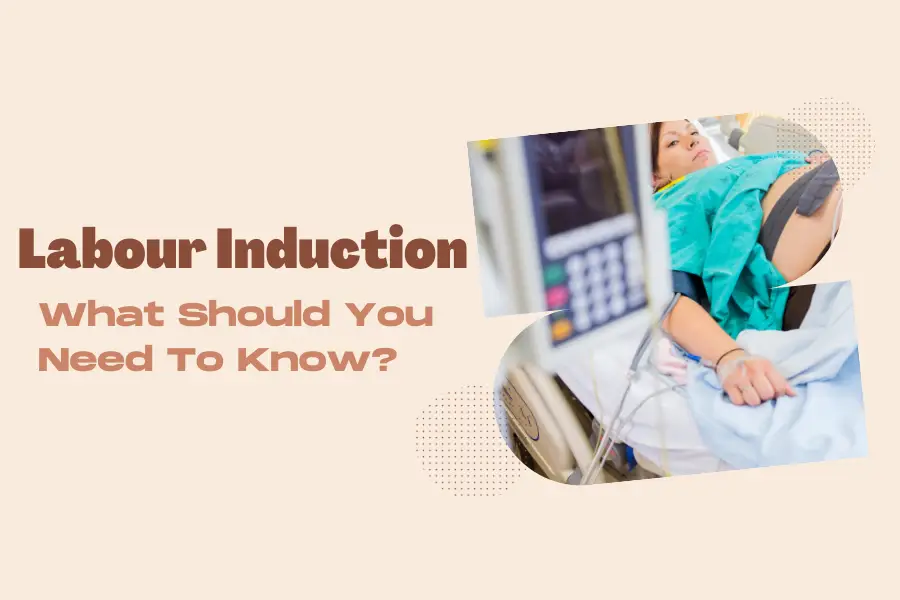
Have pregnant women ever thought about the situation that your due date has arrived but you do not see any signs of labor or your water breaks early? If those who are about to give birth figure out those situations, but do not know what to do, this is the time we will guide to labor induction.
Labor introduction is stimulating uterine contractions not naturally but must be through the intervention of a doctor. According to The Society of Obstetricians and Gynaecologists of Canada (SOGC), more than one in five laborers (over 20%) are induced, so now it is a common method for childbirth.
Understanding About Labour Induction
Labor is the progression of many phenomena, the most important of which is uterine contractions that cause the cervix to open, resulting in the fetus and placenta being expelled.
Induction of labor is a process in which the doctor creates uterine contractions to help the woman give birth through vagina. The pregnancy usually ends at 38-40 weeks. At that time, the mother will experience uterine contractions, which signal that labor has begun and the baby is about to be born. However, in this case, the mother does not have labor pain even though the due date has passed. Doctors are required to perform labor induction procedures, causing labor to end the pregnancy.
Some medical conditions such as high blood pressure, diabetes, heart or lung problems in the mother may also cause the doctor to initiate labor induction. If there are any signs of fetal distress or stillbirth, as well as if the mother lives too far from the hospital or has a history of rapid labor, the doctor may also prescribe this measure. These are just a few of the common reasons the doctor may need to perform a labour induction.
The success of the labor induction procedure for vaginal birth will depend on many factors, one of which is the degree of dilation and effacement of the cervix. The greater the opening and effacement of the mother’s cervix, the higher the likelihood of vaginal birth. The doctor may prescribe medication for pregnant women to ripen the cervix before induction of labor. This procedure is usually performed in the hospital’s delivery room to help the doctor monitor the fetus before initiating labor to ensure the fetus’s condition is stable.
Why Is Labour Induced?
To decide whether to be induced or not, a healthcare provider, doctor, or midwife will check the health of the mother as well as the baby in the mother’s womb at all prenatal appointments. This will check the mother’s cervix, evaluate the baby’s size, gestational age, weight and position in the mother’s uterus. Depending on the overall health status of the mother and baby, doctors will determine whether or not labor induction is needed.
The most popular situation that labour induction is needed is mothers who have overdue dates nearly two weeks. If you do not labour naturally by 41 weeks, the concern here is health of the placenta. Because there will be a higher risk of stillbirth or problems for the baby.
The second reason is water has broken early but no contractions. If water breaks more than 24 hours before labour starts, there’s an increased risk of infection to the baby along with the mother. And water breaks after 34 weeks, mother could choose labour of induction or expectant management.
Thirdly, while labouring, mothers may meet medical conditions, such as an infection in the uterus, low amniotic fluid, high blood pressure and placental abruption (where the placenta peels partially or fully away from the uterus wall). When these conditions happen, induction must be implemented. Moreover, there are other conditions that the mother or the baby may be suffered and lead to labour induction such as:
- Baby is growing too slowly
- Speedy, short deliveries before
- Gestational diabetes
- Chorioamnionitis (an infection in the uterus).
- Oligohydramnios (low or leaking amniotic fluid).
- Placental obstruction
Methods Of Labour Induction
Besides natural labour induction methods, such as acupuncture, breast and nipple stimulation, castor oil, herbal supplements, hot baths, eggplant casseroles and sexual intercourse, there are many surgical techniques too. So, there are various medical and surgical methods for inducing labor, and the method works for one woman or one delivery may not be efficient for another.
Membrane sweep
Membrane sweep is cervical sweep or membrane stripping. A doctor or midwife will place a gloved finger into a woman’s cervix and sweep circular motion to separate the membranes that connect the amniotic sac to the walls of the uterus. This separation releases hormones called prostaglandins to “ripen” the cervix, lead to contractions and start the labour.
The doctors or midwives also insert two gloved fingers into the cervix to open it a little more. A lot of women feel pain, but the pain just occurs in a short period. A membrane sweep is usually considered after 38-39 weeks pregnancy. If expectant mothers want to avoid medical induction and feel stressed about overdue, membrane sweep might be the right choice.
Prostaglandin
Prostaglandin is divided into 3 types: the first one is a gel put into the vagina near the cervix by the doctor or midwife, the second one is Cervidil, a tablet with an attached string put near the cervix. And the third one is a pill called misoprostol, which can be taken orally with water or put under the tongue.
With two first mentioned forms, a disadvantage is they could result in contractions that are too strong or too close together. Too strong or close contractions probably affect the baby’s heartbeat. Therefore, the healthcare providers prefer to give expectant mothers medicine to relax the uterus rather than use prostaglandins. These methods need to be administered in the hospital or an outpatient clinic and then you can go home to see if labour is going to kick in.
With the misoprostol, if mother’s bodies can metabolize it better than others, it may work better. This strategy is considered to be used if water has already broken and obstetricians worry about placing bacteria into the uterus through vaginal exams. Furthermore, among three forms the third one misoprostol causes the highest risk as too many contractions. So in this situation, mothers have to stay at the hospital to make sure that the baby can be monitored with an external monitor (mothers are allowed to move around).
Foley catheter

A Foley catheter is a thin tube with a small balloon on the end that is inserted into the cervix and inflated with water to a diameter of about two or three centimeters
This applies pressure on the cervix to open and does not result in contractions much. Also, the pregnant women do not feel the balloon inside, so they can move normally. However, the insertion can cause some menstrual-like cramping.
The pregnant woman will be observed for around an hour to make sure that there are not any signs of vaginal bleeding and the heart rate of the baby is normal. Then the mother can go home to wait for 12 to 24 hours. If labour starts sooner than expected or if the bulb falls out, it means that the balloon has finished its job to open the cervix.
In contrast, if labour hasn’t begun by the time the mother has returned to the hospital, the doctor may suggest using prostaglandins to dilate the cervix or recommend breaking the amniotic sac to start labour.
Artificial Rupture of Membranes (ARM)
Artificial Rupture of Membranes (ARM) or an amniotomy is when health providers use a crochet hook to break the amniotic sac to leak out amniotic fluid once the cervix is open enough. This procedure does not cause the pain but not be uncomfortable.
This method is usually straightforward, but the risk of cord prolapse, bleeding and infection highly increase. Therefore, ARM must be done in a hospital or clinical setting to make sure that the baby is safe.
The labour is rare to start just by breaking the waters. An amniotomy is usually performed when the cervix is in a favourable status, and oxytocin should be used after breaking the waters to ensure labour consistency.
Oxytocin (Pitocin)
Oxytocin is given intravenously or intramuscularly1. With the intramuscular (IM) route, it is easy to inject and requires less skill to administer. After an IM injection, the effect on the uterus appears within 3 to 7 minutes and lasts for 30 to 60 minutes. With the intravenous (IV) route, the uterine response is almost simultaneous within 1 min or less. Compared to the IM route, IV happens more slowly but produces a longer lasting effect23.
If used oxytocin, a pump controls the amount of oxytocin medication into the mother. The midwife will stay with pregnant women and turn up the drip every half hour until you are in labour. It can take several hours, depending on each woman. Meanwhile, the baby’s heart rate will be followed throughout labour by a CTG machine. The mothers are able to move freely by the drip and CTG machine. Oxytocin seldom leads to the uterus contraction too much. But if that situation happens, the pregnant mother will lie on their left side and the drip will be adjusted or stopped. Doctors could use another drug to reduce the contractions if their baby’s heartbeat is affected. Mothers are not capable of giving birth under the water if they choose to use oxytocin to induce labour.
The Risks Of Labour Induction

Labor induction has pros and cons. There are several risks that mothers should be aware of.
- Experience stronger, more painful and frequent contractions4.
- Increased risk of postpartum depression5.
- If labour induction fails, cesarean delivery will happen.
Additionally, labour induction possess potential risks such as:
- Infection: Certain methods of induction, such as rupturing membranes, increase the risk of infection for both the mother and the baby.
- Uterine rupture: This risk is higher for women who have had a previous cesarean delivery or other uterine surgery.
- Complications with fetal heart rate: Excessive contractions can lead to changes in the baby’s heart rate.
- Fetal death: In rare cases, induction can result in fetal death.
Induction is not suitable for mothers if they have had a previous C-section or other uterine surgery and try a vaginal birth after Cesarean (VBAC) as the risk of uterine rupture. Obstetricians advise pregnant women not to induce in some cases such as placenta is blocking the cervix (known as placenta previa), an active genital herpes outbreak, or the baby is breech or transverse (bum down or lying sideways in the uterus).
But don’t worry too much—specialized doctors will perform and oversee the labor induction. To maximize safety, the doctor will also undertake a complete examination of the mother and baby before starting labor induction. Therefore, the risk of bad situations will be better managed. It is advised that you remain composed and obey your doctor’s directions. Staying calm and focused during labor induction is very important. This might also be a good time to choose your baby boy’s name or girl’s name. Talking about names with your spouse can help you relieve stress and maintain composure throughout the birth.
Final Thoughts
Giving birth is never an easy thing, especially for mothers who are pregnant for the first time in their lives. Therefore, Babies Parent hopes pregnant mothers in addition to preparing mentally need to prepare knowledge to give birth so that both themselves and the child are healthy.
Labor induction is a process that can take place if mothers are unable to go into labor naturally. If mothers cannot go into labor on time or during pregnancy, if mother or baby or both have problems, do not worry too much because this can be intervened. And most importantly, if mothers have any concerns about pregnancy, childbirth or postpartum, see a doctor and have regular health checks to know more clearly what you need to do.
Sources
- Cotter A, Ness A, Tolosa J. Prophylactic oxytocin for the third stage of labour. Cochrane Database Syst Rev. 2007;(4):CD001808. ↩︎
- Breathnach F, Geary M. Standard medical therapy. In: B-Lynch C, Keith LG, Lalonde AB, Karoshi M, editors. A Textbook of Postpartum Haemorrhage. London: Sapiens Publishing; 2006. pp. 256–62 ↩︎
- Choy CMY, Lau WC, Tam WH, Yuen PM. A randomised controlled trial of intramuscular syntometrine and intravenous oxytocin in the management of the third stage of labour. BJOG. 2002;109:173–7. doi: 10.1111/j.1471-0528.2002.01204.x. ↩︎
- NICHD-Eunice Kennedy Shriver National Institute of Child Health and Human Development. (2012, March 30). NIH Study Finds Women Spend Longer in Labor Now Than 50 Years Ago. https://www.nichd.nih.gov/newsroom/releases/033012-time-to-labor ↩︎
- Kroll-Desrosiers AR, Nephew BC, Babb JA, Guilarte-Walker Y, Moore Simas TA, and Deligiannidis KM. Association of peripartum synthetic oxytocin administration and depressive and anxiety disorders within the first postpartum year. Depress Anxiety, 2017; 34: 137–146. doi:10.1002/da.22599 ↩︎




![[variety of unsafe pregnancy foods including raw sushi deli meat soft cheese and raw eggs on a kitchen counter]](https://babiesparent.com/wp-content/uploads/2026/03/1_Unsafe_pregnancy_foods_202603301142-768x429.webp)
